INTRODUCTION
Stroke is a common, serious, and disabling global health-care problem and many patients survived from stroke experience disabilities including gait abnormality or deficits in upper extremity control [1]. About one-third of stroke survivors live with functional limitations in activities of daily living (ADL) and life-long residual disability even after 5 years post-stroke [2,3]. Stroke-related disabilities are a serious burden to both patients, family members, and society [4]. Well-coordinated multidisciplinary stroke care including comprehensive rehabilitation and robot-assisted therapy can give a potentially beneficial treatment option for motor recovery ofthe arm and gait[1].
After neural injury such as stroke, the ability of the brain or neural network to change, named “neuroplasticity,” is the basic mechanism of functional recovery [5]. After focal ischemic brain injury, activity of remaining neural network is changed to optimize neural resources for recovery of function. During this period, inducing plasticity of neural network adjacent to the damaged area may enhance neural network reorganization and the functional restoration. The experience-dependent synaptic and circuit plasticity thatremodels synaptic buttons and connections by repeated sensory experience play the most important role. High-dose intensive training [6] and repetitive practice of specific functionaltasks [7] are essential for neural network reorganization and functionalrecovery after stroke.
During the last two decades, electromechanical or robotic technology has been developed to substitute for human actions by a reprogrammable, multifunctional manipulator to move specialized devices through variable programmed motions [8] and have been used to augment rehabilitation with greater sophistication of electro-mechanical components [9]. Robotic rehabilitation is universally well tolerated by stroke patients, and has been found to be an effective treatmentfor motor impairments after stroke. Rehabilitation using robot technology has the most important advantage of delivering high dosage and intensity intervention [10]. Because it is important to provide proper amount of errorless repetition to facilitate neural plasticity of motor system, robotic therapy became a promising technology for the rehabilitation of patients with motor disorders caused by stroke or other central nervous system disease [11]. Rehabilitation robots for stroke are usually designed to adapt forthe patient’s functional level and this process needs considerable technical flexibility. These techniques include but are not limited to passive and adaptive exercise, active assisted, active constrained and resistive exercise. The rehabilitation robot can apply constant therapy for long periods and allows for continuous monitoring of patient performance and progression that can be delivered to the therapist [12,13]. Different types of robots that can be used in rehabilitation include assistive robots that aid ADL and compensate for loss of function and therapeutic robots that provide task-specific training. Rehabilitation robots can also facilitate assessment procedures and improve their clinical value [14]. Exoskeleton as well as end-effector type robotic-assist systems were developed and applied for both gait and upper extremity motor function [12,13,15]. Exoskeletons have a structure, which resembles the human upper limb and robot joint axes match the limb joint axes. End-effector robots hold the patient’s hands or feet at one point and generate forces at the interface [16]. Robotic aids for rehabilitation hold considerable promise but have not yet achieved strong clinical recommendations [15,17]. Barriers to adoption include the limited data on efficacy, the single-purpose design of existing robots, financial considerations, and clinicians’ lack of familiarity with this technology [15]. Nevertheless, use of rehabilitation robotics has grown rapidly in recent decades, and a number of therapeutic rehabilitation robots have become available forresearch purpose and also for clinical use. In accordance with the results accumulated by new trials,there has been a quick change in clinical recommendations [14,16-23]. In this manuscript, recent research concerning robot devices forfacilitating motorfunction of both gait and upper extremities, mainly focusing on the evidence of rehabilitation for stroke patients, are described.
ROBOTIC ASSISTED THERAPY FOR IMPROVING GAIT FUNCTION
During the past decade, many articles investigating the effect of electromechanical walking-assist devices, both exoskeletal and end-effector types, on gait function of stroke patients were published. Rehabilitation robots and electromechanical-assisted training devices for stroke patient have been used to locomotion restoration. Most of these devices incorporate body weight support along with treadmills or foot platforms. It was found that the exoskeletal type of robot devices were primarily used although the end-effector type were also utilized [17]. The main advantage of robotic devices over conventional gait training is that they reduce the need for intensive therapist support. A Cochrane systematic review updated in 2017 by Mehrholz et al. [21] reviewed 36 randomized controlled studies involving 1,472 participants. They concluded that electromechanical-assisted gait training combined with conventional physical therapy increased the odds becoming independently walking (odds ratio, 1.94; 95% confidence interval [CI], 1.39 to 2.71; P<0.001; moderate-quality evidence), but did not significantly increase walking velocity (mean difference [MD], 0.04 m/sec; 95% CI, 0.00 to 0.09; P=0.08; low-quality evidence) or walking capacity (MD, 5.84 m walked in 6 minutes; 95% CI, –16.73 to 28.40; P=0.61; very low-quality evidence).
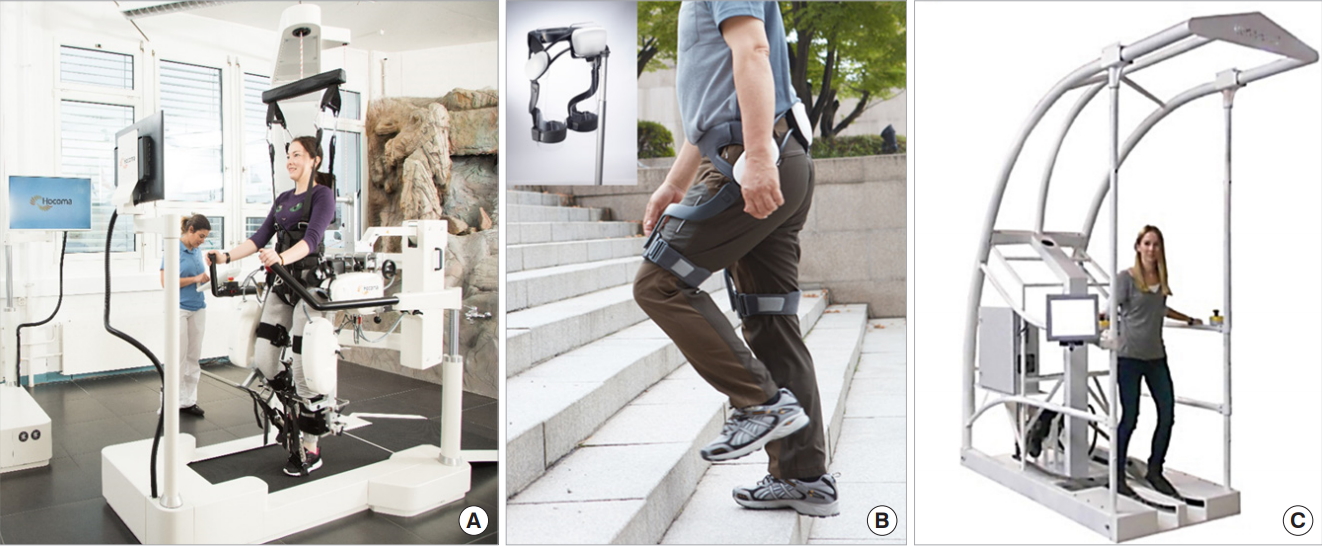
Twenty-five randomized controlled trials that investigated the use of robotic assisted therapy with exoskeleton devices for improvement of gait function in patients with stroke were selected for review (Table 1, Fig. 1A, B) [24-49]. Two studies reported superior results from robotic assisted therapy in comparison with conventional; however, both trials recruited relatively small numbers of patients. Hornby et al. [26] performed a randomized controlled trial comparing the effects of robot-assisted gait training and manual facilitation with an assist-as-needed paradigm in patients with chronic stroke. In this trial, therapist-assisted training showed greater improvements in walking ability in ambulatory stroke survivors compared with a similar dosage of robot-assisted training. Furthermore, a later multicenter randomized trial by Hidler et al. [25] investigated the effect of robot-assisted therapy on gait function in patients with subacute stroke, and concluded that conventional gait training interventions appeared to be more effective than robot-assisted gait training for improving walking ability. These two reports agreed that conventional gait therapy was more effective than robot-assisted therapy for improving gaitfunction after stroke while applied with similar training intensities. In contrast, other reports demonstrated similar or superior effects ofrobot-assisted therapy on gaitrecovery when applied in combination with conventional physiotherapy in patients with subacute stroke compared with conventional therapy alone [24,30]. Schwartz et al. [31] also concluded in a large participants study that robot-assisted gait training with regular physical therapy produced promising effects on locomotor function in subacute stroke patients than regular physical therapy. Recently, studies revealed various effect of robot-assisted therapy on gait parameters. Bang and Shin [48] reported that a robot-assisted gait training group demonstrated better performance in gait speed, cadence, step length, and balance than a conventional training group as well as reducing the double limb support period. Han et al. [38] emphasized that patients receiving robot-assisted therapy showed improvements in arterial stiffness and increased peak aerobic capacity. Kim et al. [36] demonstrated that balance, gaitfunction, and ADL were betterin a robot-assisted training group compared with a conventional training group. Taveggia et al. [37] also demonstrated better functional independence in robot-assisted treatment compared to overground treatment. In summary, robotic assisted gait therapy may not be able to replace conventional physiotherapy for improving gait function in patients with stroke but rather recommended in combination with conventional physiotherapy. Patients with subacute stage of stroke who are not able to walk independently may be more likely to experience the beneficial effect of robot-assisted therapy. However, there is still insufficient evidence on the effect of robot-assisted therapy on gait function in the chronic stage of stroke. Furthermore, specific training protocols using different types of robotic assistance to fit individual patient’s gait dysfunction may be required in the future. Exoskeletal robot assisted gait therapy for stroke hemiplegic patients also improved cardiopulmonary function compared with conventional gaittraining [24].
In contrastto exoskeletaltype robotic devices, only a small number of reports investigated the effect of end-effector type robotic devices on gait function. Nine randomized controlled trials that compared end-effector-type devices with conventional therapies were reviewed (Table 1, Fig. 1C) [33,50-57]. Six studies used end-effector-type robotic gait training in subacute stroke patients and three studies conducted in chronic stroke patients. Four of the six subacute trials demonstrated that robot-assisted gait training combined with conventional physical therapy resulted in a greater improvement in locomotor function compared with conventional physicaltherapy alone [33,51,53,54]. In contrast, only one study in the chronic phase demonstrated a positive outcome in the robotic group. Therefore, the addition of robot-assisted therapy with end-effector-type devices to conventional physiotherapy can be recommended for improving gait function in patients with subacute stroke; however, no clear beneficial effect has been found in chronic stroke patients.
In conclusion,robotic gaittraining remains promising as an adjunctive therapy to conventional gait training. To maximize the benefit of robotic gait training, further studies should be performed for patient selection, optimal device type according to the functional level, and training protocols, etc.
ROBOT-ASSISTED THERAPY FOR UPPER LIMB MOTOR FUNCTION
Robot-assisted therapy can offer large amount of upper limb motortraining for stroke patients. There are a variety of upper extremity robot types, consisting primarily of workstation devices used in a rehabilitation facility, but also including some wearable exoskeletal devices that can be used in a home environment [17]. A recent meta-analysis Cochrane review which included 45 trials (involving 1,619 participants) reported that electromechanical and robotic assisted arm training improved ADL scores (standardized mean difference [SMD], 0.31; 95% CI, 0.09 to 0.52; P=0.0005; 24 studies, 957 participants, high-quality evidence), arm function (SMD, 0.32; 95% CI, 0.18 to 0.46; P<0.0001; 41 studies, 1,452 participants, high-quality evidence), and arm muscle strength (SMD, 0.46; 95% CI, 0.16 to 0.77; P=0.003; 23 studies, 826 participants, high-quality evidence). Electromechanical and robot-assisted arm training did not increase the risk of participant drop out (risk difference, 0.00; 95% CI, –0.02 to 0.02; P=0.93; 45 studies, 1,619 participants, high-quality evidence), and adverse events were rare [23]. Twenty-four different electromechanical devices were described in the trials, which compared electromechanical and robot-assisted arm training with a variety of other interventions. Participants were between 21 to 80 years of age, the duration of the trials ranged from 2 to 12 weeks,the size ofthe trials was between eight and 127 participants and the primary outcome differed between the included trials. Furthermore, the test for subgroup differences (between acute and subacute phase after stroke versus chronic phase after stroke)revealed no significant difference (P=0.33, level of heterogeneity I2=0%).
Without a doubt this analysis demonstrated more positive outcome than previous Cochrane review [20] which revealed weaker training effect of electromechanical and robotic assisted arm training on improving ADL, arm function, and arm muscle strength due to low or very low quality of evidence. Another metaanalysis by Veerbeek et al. [19] analyzed 38 trials (involving 1,206 participants) and reported significant but small improvements in motor control and muscle strength ofthe paretic arm and a negative effect on muscle tone by robot-assisted therapy of upper extremity in stroke patients. There was no positive effect on upperlimb capacity and basic ADL.
Table 2 summarizes 32 randomized controlled trials that assessed the effect of robotic assisted therapy for improvement of upper limb motor function after stroke (Table 1, Fig. 2) [58-87]. Most ofthem used end-effectortype robotic devices with the exception of seven studies which used exoskeleton type devices. Twenty of them performed the study for the chronic stage of stroke patients, 10 for the subacute phase, one for the acute phase, and one was undetermined. Electromechanical and robotic assisted arm training did not improve the risk of participant drop-out, but adverse events were rare. Each study used a diverse protocol and intensity of therapy; therefore, no uniform conclusion can be drawn. Indeed, more detailed analysis is needed to develop guidelines for individual stroke rehabilitation. Eleven studies reported better outcomes in upper extremity motor function compared with conventional treatment. A study by Fasoli et al. [61] consisting of 56 patients with subacute stroke reported that patients who received conventional therapy alone showed little improvement, whereas patients who received robotic training plus conventionaltherapy using end-effector type devices continued to improve in the latter half of the inpatient rehabilitation period. A study by Lo et al. [65] that recruited 127 chronic stroke patients reported that robot-assisted therapy and conventional therapy produced similar amounts of improvement after 12 weeks of treatment. However, after 36 weeks of therapy, the robotic assisted therapy achieved greater motor improvement than conventional therapy. Hsieh et al. [75] applied robotic devices with constraint-induced movement therapy and reported significantly increased Fugl-Meyer Assessment (FMA) scores in the robotic training group compared with the conventional therapy group and also found significantly better improvements in upper limb motor function in the higher-intensity robotic assisted training group [88]. In contrast, motor recovery of upper extremity did not significantly different between the lowerintensity therapy and the control groups. These results suggestthatthe therapy intensity is the important variable of robot-assisted therapy for upper extremity motorrecovery in chronic stroke patients. Two studies with subacute stroke patients suggested that additional robotic therapy showed greater improvements in ADL [61,69]; however, trials in chronic stroke patients demonstrated no additional improvement in ADL [63]. Eight trials used exoskeleton type robotic devices for upper extremity motor function in patients in the chronic stage of stroke. Fazekas et al. [89] reported a significantly better effect on spasticity in the robot-assisted therapy group than in the conventionaltherapy group. Other reports demonstrated no significant difference between robot-assisted therapy with exoskeleton devices and conventional therapies [27,29,83,90]. Therefore, the assisting effect of robotic devices on ADL was insufficient to draw a definite conclusion until the recent meta-analysis Cochrane review was published [23].
In summary, people who receive electromechanical and robotic assisted arm training after stroke mightimprove their ADL, arm function, and arm muscle strength; however, there were variations between the trials in the participant characteristics, measurements used,therapy types, and the intensity, duration, and amount of therapy. Moreover, further studies are needed to draw a definite conclusion whetherthe improving effect of robot-assisted training transferred to facilitating activities in real world for patients with stroke.
ROBOTIC ASSISTED THERAPY FOR HAND MOTOR FUNCTION
Eight randomized controlled trials using robotic devices for improving hand motor function of stroke patients were included in this review (Table 3) [22,91-98]. The type of robot and participants’ characteristics were diverse; six ofthem applied end-effector type devices and three of them used exoskeleton type robot devices. Six ofthem performed the study for patients in the chronic stage of stroke, two for subacute stroke, and one undetermined stage. The outcomes ofrobotic assisted therapy on hand motor function were also variable; four studies out of nine demonstrated superior effects of robotic assisted training on hand motor function in comparison with conventional therapy for stroke patients and the remaining five studies did not demonstrate better functional outcome of robotic therapy. Three studies used exoskeleton type devices, two of which demonstrated a favorable effect in chronic stroke patients [96,98]. Out of the six studies that used end-effectortype devices, only two showed favorable outcomes. Hwang et al. [93] demonstrated that end-effectortype robotic assisted therapy provided dose-dependent improvements in hand function of chronic stroke patients. However, the trial was a single-center study with a relatively small number of participants. Orihuela-Espina et al. [95] reported positive results of robotic training in hand motor performance and FMA scores in the subacute stage of stroke. Other studies did not find significant differences between the robotic training group and the conventionaltherapy group in both FMA and hand dexterity test results. A recent study by Villafane et al. [22] also reported that robotic assisted mobilization performed in conjunction with traditional physical and occupational therapy showed no additional effect to the traditional rehabilitation in the treatment of pain and spasticity in hand paralysis after stroke. Well-designed large randomized controlled studies are needed in order to investigate the effect of electromechanical or robotic assisted therapy on hand motorfunction and ADL of patients in different phases of stroke.
CONCLUSION
The results of well-designed studies using robotic devices for gait and motorfunction has resulted in changes to the description for practice guideline in stroke rehabilitation. Many reports have described the efficacy of robot-assisted therapy for improving gait and upper extremity motor function in patients with stroke. However, there is still a remarkable heterogeneity of the robotic devices and the participants’ characteristics as well as the diversity ofthe study designs in the literature.
Electromechanical or robotic assisted walking devices was found to be more effective than conventional gait training at increasing early independent walking after stroke and could be considered for patients who would not otherwise practice walking. However, they should not be used in place of conventional gait therapy [17,18,21]. Overall, the role of robotic assisted gait therapy in stroke rehabilitation is an adjunct to rather than a replacement for conventional rehabilitation therapy. Electromechanical and robotic assisted arm training improved ADL, function, and muscle strength of the affected arm in people after stroke. Although there were variations between the trials in the intensity, duration, and amount of training, type of treatment, participant characteristics, and measurements used,the quality of evidence was high [23].
Robotic assisted therapy for stroke rehabilitation has achieved remarkable advances in recent decades and will be further advanced with collaboration of the fundamental elements of the forth industrial revolution such as artificial intelligence (AI) and internet of things (IoT) in the near future. Ongoing improvements of the related technology may enhance the clinical efficacy and economic efficiency of such devices. Such advances will lead robotic assisted therapy to being a standard therapeutic modality in stroke rehabilitation [11].