INTRODUCTION
Fibromuscular dysplasia (FMD) is a non-inflammatory and non-atherosclerotic disease of unknown cause which affects the small- and medium-sized arteries. The most commonly involved blood vessels are the renal and cervicocephalic arteries. If the disease involves the cervicocephalic arteries, it can cause abnormalities, including carotid and vertebral artery stenosis, arterial dissection, and aneurysm formation [1-3].
FMD is definitively diagnosed by imaging studies such as computed tomographic angiography (CTA), magnetic resonance angiography (MRA), and digital subtraction angiography (DSA) [2]. High-resolution magnetic resonance imaging (HR-MRI) techniques have recently been introduced to clinical practice, and provide a high value for the etiological diagnosis of intracranial arterial diseases [4-7]. Here, we report patients diagnosed with cervicocephalic FMD who underwent HR-MRI. To our knowledge, this is the first case report of HR-MRI in a patient with intracranial FMD.
CASE REPORT
Case 1
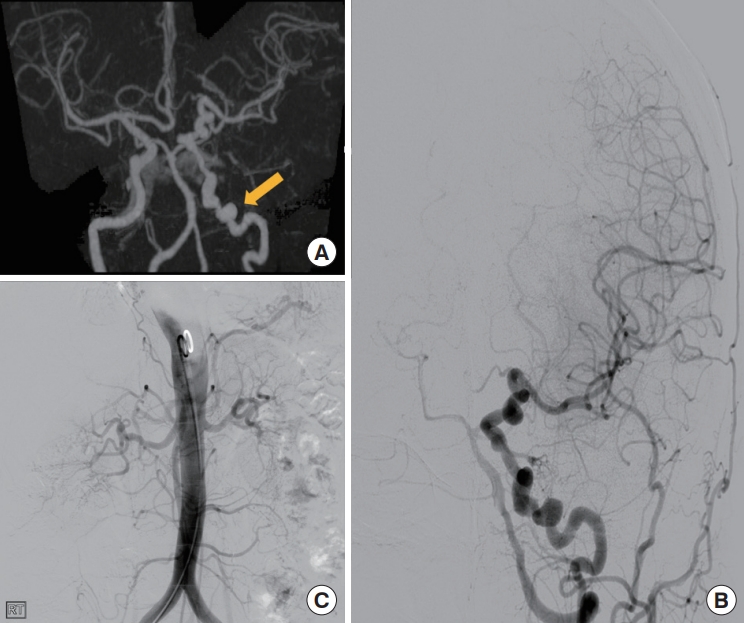
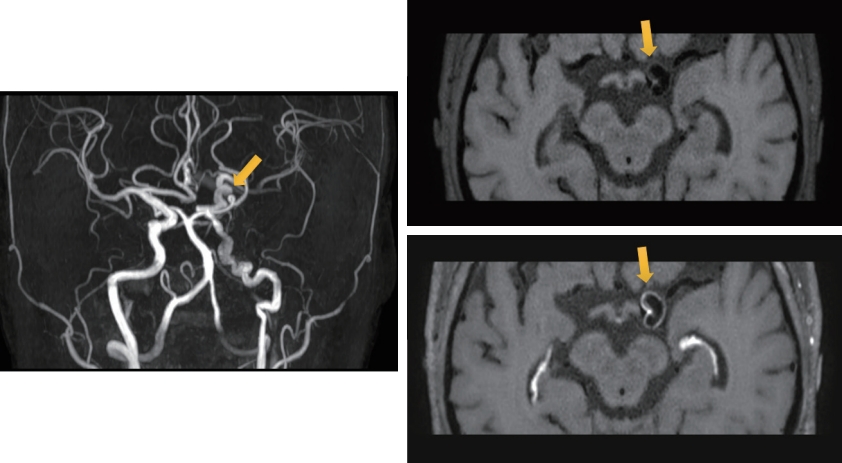
A 60-year-old previously healthy woman was admitted with short-term vertigo lasting a few seconds. Vertigo was aggravated by positional changes and improved with bed rest. Initial neurological examination results were normal. She was diagnosed with benign paroxysmal positional vertigo as the cause of symptoms. Brain CTA showed multiple stenoses and dilatations with a string-of-beads appearance in the left internal carotid artery (ICA) (Fig. 1A). The patient was admitted to our hospital for DSA. In the left common carotid artery angiogram, vessel tortuosity and a string of beads were observed from the left petrous portion to the ICA bifurcation, a typical luminal feature of FMD (Fig. 1B). Aorta angiography revealed normal renal arteries bilaterally (Fig. 1C). HR-MRI revealed concentric wall thickening and saccular enhancement with dystrophic calcification in the distal segment of the left ICA (Fig. 2). Aspirin was prescribed at discharge, and she had no symptoms for up to 6 months after discharge.
Case 2
A 42-year-old, previously healthy woman visited our hospital with headache and shoulder pain. Initial neurological examination results were normal. She underwent brain MRI and MRA to rule out secondary headache. MRA of the brain further revealed dilatation and tortuosity of the right ICA (Fig. 3A). HR-MRI was performed for further evaluation, and aortic CTA was performed to identify any renal artery involvement. No stenosis or aneurysmal dilatation was observed in the renal arteries (Fig. 3B). HR-MRI revealed diffuse wall thickening but no enhancement in the right ICA from the petrous portion to the distal communicating segment (Fig. 3C, D).
Written informed consents by the patients were waived due to retrospective nature of our study.
DISCUSSION
Intracranial arteries are involved in 7% to 20% of cases of cervicoencephalic FMD [8]. Most cervico-encephalic FMD are located in the ICA, most commonly in the middle or distal segments. Vertebral artery involvement is less frequent and generally co-exists with carotid lesions. In addition, 50% of patients with carotid artery lesions have renal artery disease [9].
Our patient presented with headaches and vertigo. In the United States registry for FMD, 60% of patients experienced significant headache [10]. Pulsatile tinnitus is another common symptom of FMD. Dizziness may occur in one quarter of the patients, but true vertigo is uncommon in FMD. The most disruptive sequelae of cerebrovascular FMD include transient ischemic attack, stroke, subarachnoid hemorrhage, and cervical artery dissection, which have been reported in 13%, 10%, 1.1%, and 12% of patients, respectively [10]. Severe stenosis producing cerebral hypoperfusion, thromboembolism, dissection, and aneurysmal rupture could be mechanisms of focal neurological events. Treatment of FMD patients depends on the particular neurological symptoms and complications [8]. In this study, patients asymptomatic, and there were no vascular complications such as dissection and aneurysm.
The pathological classification of FMD is based on the dominant vessel wall layer, intima, media, and adventitia. Among the three pathological FMD types, the media type is the most common, accounting for more than 85% of cases [1,10,11]. Medial fibroplasia shows multifocal stenosis, termed the ‘string-of-beads; appearance, while intimal fibroplasia shows focal stenosis [3]. The cases presented in this report were classified as having media-type FMD involving intracranial ICA. Medial FMD presents as alternating areas of thinned media and thickened fibromuscular ridges in which the arterial muscle is replaced by fibroplasia with loose collagen [11].
In this series, HR-MRI of the first case showed concentric wall thickening and saccular enhancement, whereas the other case showed no enhancement. The clinical implications of vascular enhancement in FMD remain unclear. In cases with carotid web, also known as carotid intimal variant FMD, previous studies have shown that HR-MRI reveals protrusion with enhancement along the posterior margin of carotid bulb [12]. HR-MRI feature of concentric wall thickening may be related to the pathological features of thickened fibromuscular ridges. In addition, the HR-MRI findings of concentric enhancement with wall thickening in our case were similar to those of patients with symptomatic moyamoya disease [6]. Therefore, diffuse concentric enhancement within vessels could represent hyperproliferation of the vessel wall components and may be related to symptomatology in FMD. Further studies are needed to determine whether HR-MRI can provide information about the natural course of FMD.
In conclusion. HR-MRI can be used to directly visualize vessel walls. As the natural course of this disease varies among patients with FMD despite similarities in luminal features, further studies with HR-MRI are needed to test the diagnostic and prognostic role of HR-MRI in patients with FMD.